
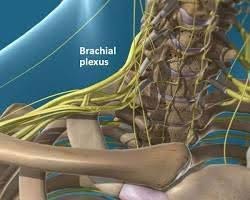
Arthroscopic Rotator Cuff Repair (ARCR) is commonly performed along with other procedures during the same surgery to ensure comprehensive treatment for shoulder injuries. This operation is typically done under General Anesthesia with a Brachial Plexus nerve block (Interscalene, Suprascapular, or Axillary). An anesthesiologist will explain the risks and benefits to you prior to the procedure. The nerve block is usually performed with ultrasound guidance before or after general anesthesia and helps with post-operative pain management.
Type of Surgery:
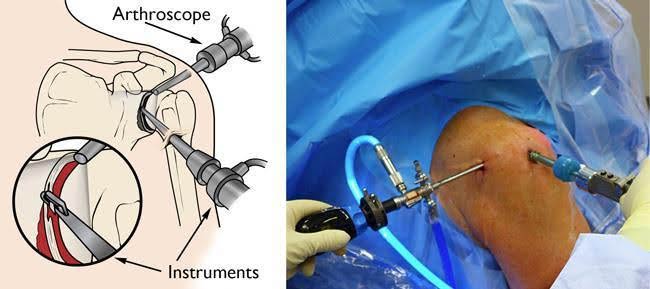
1. Arthroscopic Portals
The portal is an incision where the camera and surgical instruments are passed through the skin into the shoulder. The portal is typically around 1 cm in size, with the number of portals depending on the specifics of the procedure. Generally, 3-5 portals are used.
2. Rotator Cuff Repair
The procedure begins by identifying and debriding the rotator cuff tear, including the tendon involved, the number of tendons affected, tear configuration, retraction degree, and tendon tissue quality. These details are analyzed and classified, which guides the repair technique and pattern.
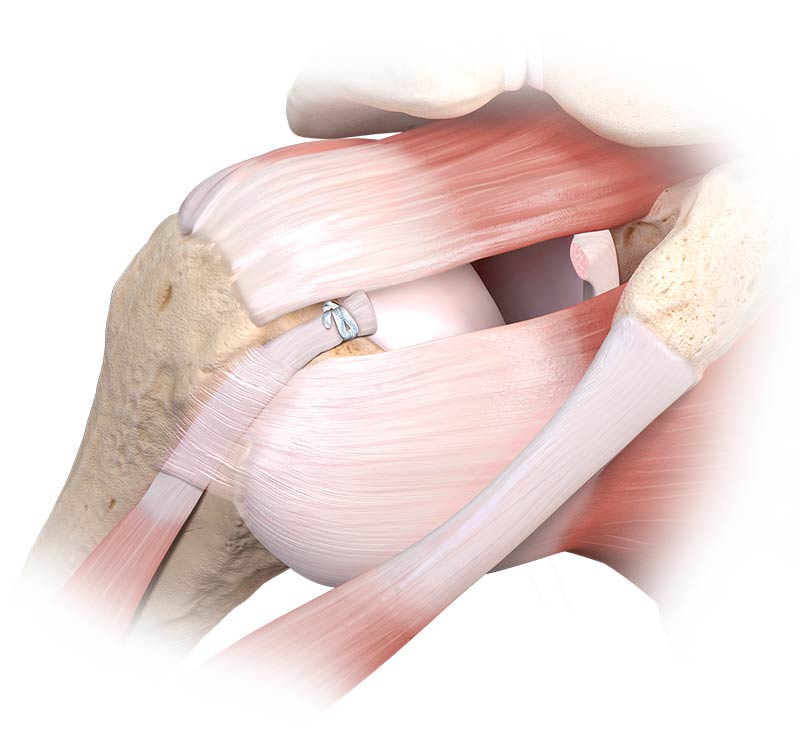
Single-row vs. Double-row Repair:
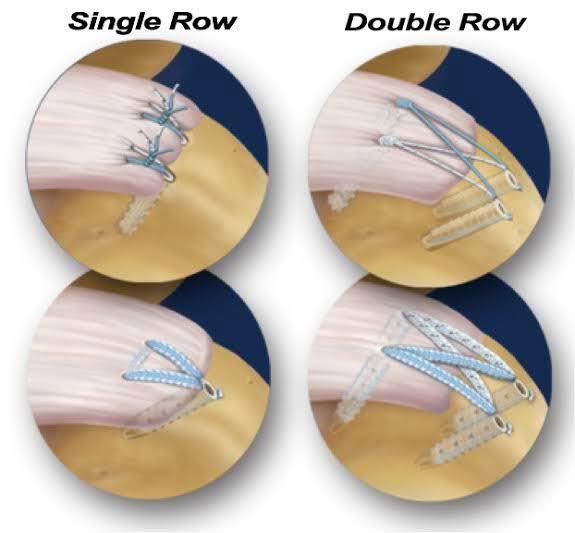
From the above pictures, you can see a larger contact area of the tendon repair site from the Double row repair, which provides potential advantages in biomechanics. By the way, there is no clear-cut winner since the clinical evidence is not entirely conclusive.
Double row repair will be achieved with 3 major factors; good bone quality of the anchoring area, proper tension of rotator cuff tissue and good quality of rotator cuff tissue. Without all of these 3 qualifications, Single row repair is my choice.
In conclusion, the decision between single-row and double-row should be made on a case-by-case basis, with careful consideration of the risks and benefits.
3. AcromioplastyAs illustrated in this infographic from Arthroscopy Journal, acromioplasty is commonly performed with rotator cuff repairs, especially in cases of a hooked or curved acromion. This procedure, which takes only a few minutes, reduces the mechanical causes of rotator cuff tears (impingement), improves surgical visualization, and may have biological benefits by releasing growth factors from the bony surface.

4. Acromioclavicular Joint ResectionAcromioclavicular joint arthritis is another condition that may be related to rotator cuff syndrome. It can cause pain when moving the shoulder, particularly during elevation or cross-body adduction. An arthritic bone spur can also impinge on the rotator cuff tendon.
This additional arthroscopic procedure takes approximately 10 minutes. It is primarily
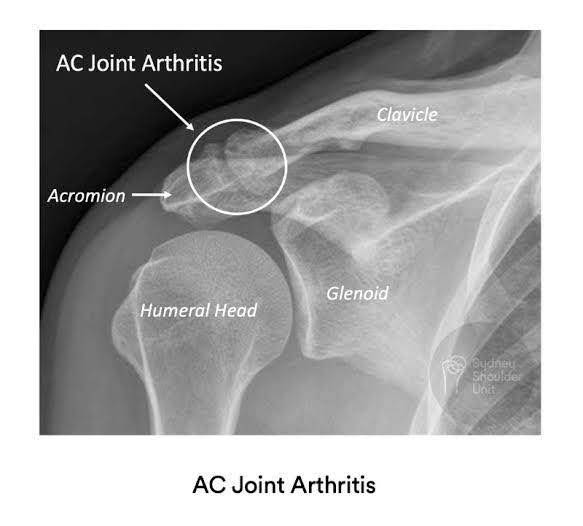
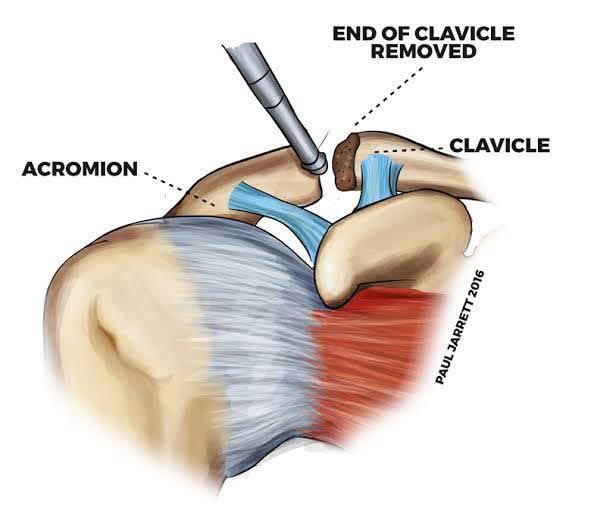
considered based on clinical symptoms and secondarily on MRI findings indicating impingement caused by the arthritic spur.
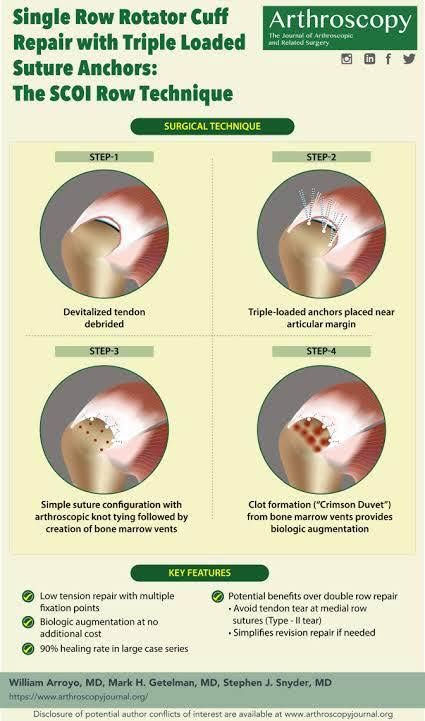
5. Crimson Duvet Procedure (Microfractures in the Bone at the Tendon Attachment Site)The Arthroscopy Journal infographic explains this procedure in more detail. I routinely perform the Crimson Duvet procedure during arthroscopic rotator cuff surgeries to provide biological augmentation, which results in better surgical outcomes.
6. Capsular Release and Rotator Interval Resection
These procedures are used to treat shoulder joint stiffness (frozen shoulder), improving the range of motion. Rotator cuff disorders and Adhesive Capsulitis (frozen shoulder) are interrelated—one can lead to the other.
Consideration for these procedures depends on clinical signs and symptoms, pre-operative or intra-operative physical examination, and operative findings of joint capsule thickening. In my experience, more than half of rotator cuff patients also have Adhesive Capsulitis and require varying degrees of soft tissue release. These procedures alone can provide excellent outcomes in cases of pure Adhesive Capsulitis.

7. Biceps Tenotomy / Biceps Tenodesis
The long head of the biceps tendon, located inside the shoulder joint, can cause issues such as inflammation, tears, and subluxation.
- Biceps Tenotomy: A simple procedure where the tendon is cut at its attachment point in the shoulder and allowed to retract into the upper arm. This may lead to a “Popeye deformity” (visible bulge) and potential muscle cramping, especially with heavy lifting.
- Biceps Tenodesis: In this more complex procedure, the tendon is cut and reattached to a different location on the humerus (upper arm bone). This involves a longer recovery period.
Tenotomy is typically recommended for elderly patients with more fatty arms who require quicker recovery. Tenodesis is more appropriate for younger, muscular patients or those who engage in heavy lifting.
8. Superior Capsular Reconstruction (SCR)
SCR is used to treat massive, irreparable rotator cuff tears that cannot be repaired using traditional suture techniques. The procedure reconstructs the weakened or torn superior capsule of the shoulder joint, which is crucial for stabilizing the joint and centering the ball within the socket.
This procedure is usually performed for large, irreparable rotator cuff tears. My first choice of graft is the long head of the biceps tendon, as it is already in the surgical area and can be re-routed or re-attached to reinforce the remaining rotator cuff tissue. If the biceps tendon is not suitable (e.g., due to a tear at the glenoid origin or a SLAP tear), I prefer to use synthetic materials or dermal patch grafts to restore joint stability.

